Goddess
-
Posts
9,970 -
Joined
-
Last visited
-
Days Won
93
Content Type
Profiles
Forums
Events
Everything posted by Goddess
-
-
 Neither The Alberta Prosperity Project, nor Stay Free Alberta has been named.
Neither The Alberta Prosperity Project, nor Stay Free Alberta has been named. -
CBC's own investigation revealed that the disinformation campaign around Alberta separatism largely came from click farmers and YouTube operators in the Netherlands...content creators chasing ad revenue by hiring actors and pumping out sensational videos. Meanwhile, the RCMP has told the Alberta government that, as of April 2026, they have found no credible evidence of foreign interference in the provincial separatist movement. Yet on CBC, Dragons' Den investor Arlene Dickinson insisted there is Russian disinformation at work. When she said, "I find that very difficult to believe... that there's no foreign interference in this," CBC anchor Andrew Nichols offered no pushback. The network's own reporting on the Dutch operators did not substantiate the kind of coordinated foreign interference she implied. This echoes CBC's coverage of the Freedom Convoy, where figures like Justin Ling pushed narratives of extremism and foreign interference with little hard evidence at the time—narratives that politicians and officials later cited as "proof" during the public inquiry. It feels like another CBC-driven frenzy. Arlene Dickinson's certainty aside, the stakes here go far beyond a few protesters on Parliament Hill. This concerns an entire province's grievances and future. Painting legitimate discontent as the product of foreign puppets risks alienating people further rather than addressing root issues. Brodie Fenlon, as Editor-in-Chief, it might be time to dial back the hype and stick closer to the facts on the ground. Good gawd, you people just swallow whatever the Liberals and the CBC tell you to. 🙄 Like how the fuque would Arlene Dickinson know?

-
Alberta, where Canada’s doom will be decided
Goddess replied to paxamericana's topic in Federal Politics in Canada
🎶 Don't you.......forget about me. 🎶 -
Meme/Cartoon of the Day
Goddess replied to WestCanMan's topic in Federal Politics in the United States
-
Meme/Cartoon of the Day
Goddess replied to WestCanMan's topic in Federal Politics in the United States
-
I hope this is a parody account, but I suspect it's not.

-
This one is my favourite 👇 If the Cultist Narrative Network/Cultist Broadcasting Corporation gave an infinite number of monkeys an infinite number of typewriters, leftists would believe everything they typed.
-
Would be nice if the media would investigate THIS foreign interference: English Cover_2024 The fact that MP colleagues needed to be "reminded" of their oath to Canada, is a good indication of why we are now facing these tariffs...
-
One of the sponsors of the Alberta foreign interference report that came out yesterday, and that the media are now running with, is the Canadian Digital Media Research Network. Guess who sponsors them? The Government of Canada. Enjoy your PSYOP.
-
Do you? You're the one who voted for more of the same.
-
Yeeeesssssss. Everyone who wants fiscal responsibility from the government is a total loon. 🙄
-
Lots of Alberta separation questions answered here: Value_of_Freedom-DraftFiscal-Plan-10July2025.pdf
-
Conservatives just introduced 3 MAJOR initiatives for new parents in Canada: Parents could return to work WITHOUT losing parental benefits and use the remaining time later. Parents could go back to school while receiving parental leave. Parents could earn income caring for children, seniors or sick family members WHILE still receiving benefits. This is the type of policy Canadians have been begging for. Flexible. Practical. Pro-family. Pro-worker. OR: We can put ANOTHER $13 billion on the country's credit card and give it away to unaccountable bureaucracies for climate initiatives.
-
-
Why not? Canada doesn't want to be great. Canada just wants to help every other country besides their own.
-
RCMP found no evidence of foreign interference in Alberta separatist movement, minister says - The Globe and Mail Won't stop the ding-dongs here from repeating the original lie for the next 10 years, much like they did with the supposed Russian interference with the Convoy. Donald Trump? RUSSSIA! Freedom Convoy? RUSSIA! Alberta separatists? RUSSIA! Anything critical of the Liberal party, the media brands as "Russian interference." Who believes this shit anymore?
-
Alberta has more resources than just oil. And we would have the freedom to develop them better. Canada is signed on to the UN Convention on Transit Trade of Land-Locked Countries, wherein it is mandated that land-locked countries have the right to transit goods across the territories of transit states to or from a coastal port.
-
I see a lot of comments online about "If Alberta separates, I'm moving there." Nope. When Alberta is gone, there will no longer be a Conservative party. The rest of you will have Liberal governments in perpetuity. You will continue to be taxed into oblivion, only for that money to go overseas to gender-sensitive rice farmers in Viet Nam and tranny bean farmers in the Congo and to Ukraine. You will continue to pour money into Carney's Net Zero agenda, long abandoned by the rest of the world. We don't want your sorry a$$es, save yourselves like we had to do. The October referendum - it's not just about separation, a lot of questions about immigration. Nope. Not taking in charity cases who rob us blind any more. Albertans don't see Canada getting better, only worse. We stand a better shot on our own, come what may.
-
Alberta, where Canada’s doom will be decided
Goddess replied to paxamericana's topic in Federal Politics in Canada
We've had Ottawa over a barrel for decades and they've ignored us. Prairie separation is no longer about leveraging a better deal with Ottawa. Those days are over, Ottawa has refused. We get it. It's about not going down with the Titanic at this point. We also don't care that anyone calls us "traitors" for getting into the lifeboats. Not one f*cking bit. -
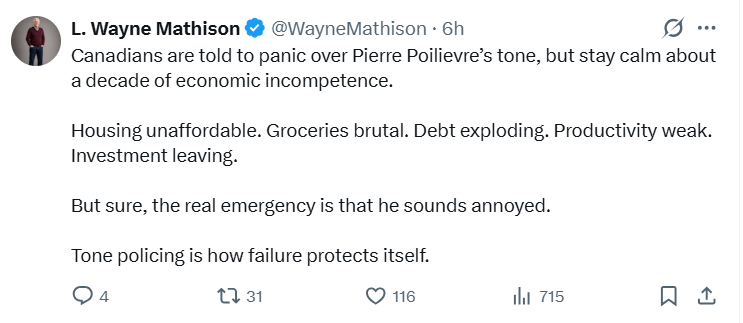
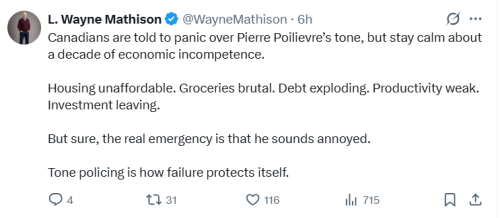
Every time I see this argument from him, I think back to the not-so-olden days rape trials where the woman was grilled about "Well, WHAT WERE YOU WEARING?"
-
Q-958 (45-1) - Written Questions - House of Commons of Canada Since 2015, the asylum claimant backlog (i.e. people who are eligible for the IFHP) has surged from 9,999 to over 295,000. This backlog largely resulted from Liberal government policies that included lifting the visa requirement for Mexico, allowing non-citizens to illegally cross the border and claim asylum, and a flood of claims from foreign students whose permits had expired. This meant that the cost for running the IHFP rose from $66M in 2016 to a projected $1.5B in 2029-30, or, a 2194% increase. This has placed an unacceptable level of strain on Canadian healthcare. More than 100,000 Canadians have died waiting for care since 2018 6 million Canadians, 1 in 5, lack access to a family doctor Wait times to see a specialist are over 28 weeks (7 months). Each of these visits put on the system via the IHFP are an additional demand on the already overburdened Canadian healthcare system. This is why earlier this year, Conservative brought forward a motion to restrict health care access for failed asylum claimants to emergency life-saving care only. The proposal maintained emergency, life-saving care and an equal standard for denied claimants, as well as non-discrimination based on country of origin. The proposal was defeated by the Liberals.
-
Remember when the Liberals said Poilievre would cancel Pharmacare, but THEY would keep it? Canada healthcare: Some shocked feds won't sign pharma deals Health advocates shocked as Carney Liberals back away from pharmacare program