Goddess
-
Posts
10,058 -
Joined
-
Last visited
-
Days Won
93
Content Type
Profiles
Forums
Events
Everything posted by Goddess
-
This has been explained to you many times. It does not require tens of thousands of people to pull off something like this. It just requires a handful of people who then rely on useful id10ts, like yourself. I have an 82-page thread with hundreds of peer-reviewed studies and links to official data from all over the world, emails/text trails, etc from FOIPing and documents that have been handed over by whistleblowers. You have CBC headlines.
-
Probably way over your head, and you won't read it anyways, but I'll post just one of the scientific rebuttals: A Step-by-Step Evaluation of the Claim That COVID-19 Vaccines Saved Millions of Lives Short version: 1. "Millions saved" came from computer models, not real data. Computer models, which were stacked with assumptions, ignored natural immunity and excluded harms. Political projections, not science. 2. The "Stop the Spread" lie. The models only worked because they assumed the shots stopped infection and transmission. Breakthroughs happened within weeks and the boosted were driving the waves, due to OAS. The core input was false. 3. Zero proof of deaths prevented. When transmission collapsed, the narrative shifted to "it prevents death." Yet RCT's showed no mortality benefit. There were 15 deaths with Pfizer, 14 in the unvaccinated group. 4. Manufactured myth. With no evidence, officials and media enforced the story with methodological tricks, cherry-picking, dashboard spin and censorship. CONCLUSION: The "millions saved" line is the fraudulent fallback of the Pharma cartel. It isn't science. It's propaganda.
-
 South Korea former president JAILED for enacting martial law unjustly. Just sayin' South Korea’s former prime minister jailed for 23 years in martial law case | CNN
South Korea former president JAILED for enacting martial law unjustly. Just sayin' South Korea’s former prime minister jailed for 23 years in martial law case | CNN -
It doesn't. Sorry, but it just doesn't.
-
Well, they would have been threatened with having their licenses revoked, as happened to the docs and scientists who DID point out that we were not following any of the official pandemic protocols or the science. Also I doubt your doctor is too involved in Emergency Planning on any level or had any knowledge of what the pandemic protocols are/were. Hard to say something about which you know nothing. (Although you do it all the time.) Yes. Again, because there were issues yet to be resolved with the technology, despite the decades of research. I understand why you think that. You get your info from CBC and have extremely little knowledge of how the immune system works. Millions of lives were never in any danger, so you can't really claim them as being "saved."
-
I think it does. At best, it's a problematic parallel.
-
And you are.......?? Who??
-
I see. So you have nothing. Thanks.
-
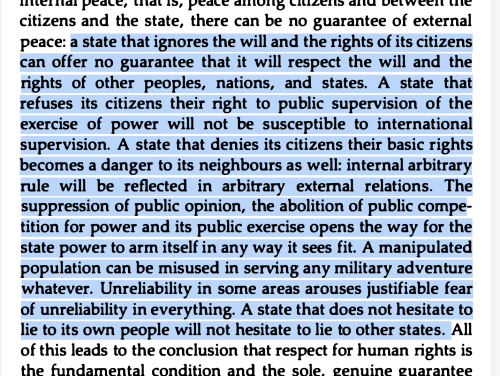
It was eloquent, yes. It didn't have his usual "uhhhhh"s and "ummmm"s peppered throughout it. I'm not sure he really understands Havel's The Power of the Powerless, though. I feel like he misapplied it. And he definitely didn't read this part from "Living in Truth":
-
I keep seeing this, but I can't find either an arrest for or a conviction for pedophilia, involving Trump. Can you please provide a cite for this claim?
-
Carney's speech was clearly to create fear of Trump. I suspect the Liberal slogan for the next election will go from "Elbows Up!" to "Poop your pants!"
-
No, it's not a good thing. I covered this in the Trickle Thread - why pandemic experts have always said NOT to vaccinate during a pandemic. Yes. Despite decades of research, they were never brought to market before. For a reason. Those reasons were not resolved before the covid pandemic. Hopefully, scientists like Dr. McKernan can resolve the issues and make them safer so we have less Kayla Pollacks, less Sean Hartmans next time. It had an IFR of slightly higher than the seasonal flu, a 99.9% survival rate and was only risky for a very tiny percentage of the population. Bad time to try out 2 technologies that never made it past the testing stage.
-
I found this Op-Ed, by Cosmin Dzsurdzsa of Juno News, quite enlightening. He discusses the Canadian "cartels" dominated by old, moneyed family dynasties that are running things - Rogers & Shaw in telecommunications (The Digital Services Act), the Irvings (oil & shipbuilding), the Westons (retail). He points out how every sticking point in our current CUSMA trade disputes with the US can be understood through this lens. See what you think: Dear Americans, Canada is run by powerful Cartels Canada as a nation is not particularly difficult to understand if you spend even a small amount of time thinking about how the system actually operates and I think the Americans are starting to catch on. It goes like this: Canadian governments exist, to varying degrees, largely as protectionist rackets with the sole purpose of preserving a series of entrenched industry monopolies and cartels. These cartels are largely dominated by a small number of old, moneyed family dynasties (the Rogers and Shaws in telecommunications, the Irvings in oil and shipbuilding, the Westons in food retail, and many others). For simplicity’s sake, I’ll refer to these powerful, dynamic industry groups as “The Cartels” going forward. This is the basic operating theory of Canadian politics. Once you understand it, almost everything else begins to make sense. Nearly every sticking point in Canada’s ongoing USMCA trade disputes with the United States can be understood through this lens (more on that shortly). First, it’s worth exploring the broader implications of this operating theory. The implication is that virtually every piece of legislation, every policy choice made by the government-of-the-day, and every trade relationship is viewed internally as a zero-sum game: net gains or net losses for The Cartels. The public interest is often secondary and incidental. Canadian governments win or lose elections and sometimes tear themselves apart based on how well they balance the sometimes competing interests of The Cartels. Some of The Cartels are more closely aligned with Conservative governments, others with Liberal ones. But the most powerful and deeply entrenched of The Cartels almost always emerge unscathed, regardless of which party is in power. By far, the Liberal party, often self-indulgently described by Canada’s Laurentian elites as the country’s “natural governing party” has proven the most adept at protecting cartel interests. The Liberals excel at this game because they understand how to obscure the underlying reality: that laws and decisions are made primarily to protect monopolies, by wrapping those decisions in branding that appeals to Canadian identity, culture, sentimentality, or phoney nationalism. Take dairy as a clear example. For those unaware, dairy and other agricultural goods in Canada are determined by a supply management system, essentially a central planning system where bureaucrats determine quotas, supply and dictate pricing. Supply management has been a persistent flashpoint in USMCA negotiations. U.S. President Donald Trump has personally called out Canada’s "250% tax" on dairy products, and American negotiators have repeatedly pushed to put dairy access on the table, much to Ottawa’s chagrin. Why won’t Ottawa budge? The answer is simple: the dairy cartel. Within Canada, and especially within Conservative circles, much has already been said about the outsized political influence of the dairy cartel across both major federal parties. Anyone who witnessed the 2017 Conservative Party of Canada leadership race will quickly see how radioactive this issue became (but that is a separate can of worms best left unopened here). What matters is that the dairy cartel is not merely influential; it is legally entrenched. Entire statutory frameworks and government bodies exist, namely the Farm Products Agencies Act and the Canadian Dairy Commission, solely to serve their interests. This is cartel behaviour, formalized by law. Now consider the Digital Services Act. As recently as yesterday, U.S. Secretary of Commerce Howard Lutnick explicitly raised this issue while speaking at the World Economic Forum, calling out Canada’s insistence on taxing U.S. digital products. What’s notable is that opposition to Canada’s digital taxes has been bipartisan in the United States. Even the former U.S. trade representative under Democratic President Joe Biden, Katherine Tai, expressed frustration with Ottawa’s approach and requested dispute settlement over this issue. On this particular tax, Canada has retreated and recently rescinded the tax. But the question remains: why did Canada fight tooth and nail under threat of tariffs and consequences to preserve this tax? Because of the media and telecommunications cartel. The Digital Services Act is only one iteration of an entire web of legislation and trade policy designed to preserve the media/telecoms cartel. The Digital Services Act, the Online Streaming Act, and the Online News Act are all part of the same architecture. These laws are the reason Canadians can no longer access news on Facebook to this day. The media/telecom cartel, organized through lobbying groups such as News Media Canada, successfully pushed these measures through under the guise of fairness and cultural protection. But the underlying reason is far less flattering: Canada’s legacy media sector cannot compete with American firms due to chronic deficiencies in talent, innovation, scale, and human capital. Without protection, subsidization, and forced revenue transfers, the system collapses. The reason I highlight dairy and media/telecom specifically is not only because they are central to Canada’s trade disputes with the United States, but because they illustrate how effectively the Canadian government has sold these protectionist regimes to voters. Supply management is framed as a patriotic necessity. Canadians are told that dairy farmers must dump millions of litres of milk down the drain each year to meet quota targets because Canadian dairy is inherently superior to American dairy. Media subsidies and telecom monopolies are justified as essential to preserving culture, heritage, and a disingenuous "Canadian nationalism." Any appeal to preserving Canadian sovereignty should at this point be considered an appeal to preserving the system of The Cartel I have just laid out for you. These narratives work. They ensured compliance. And it certainly helps that Canada’s media ecosystem itself is thoroughly monopolized (a point I have addressed at length elsewhere). So you see, the system is actually quite simple. The same logic applies to many of Canada’s most questionable laws and trade practices. And to return to my original point: I think Americans are beginning to understand this faster than Ottawa likes to think. For years, Canada’s Laurentian elite appeared to believe they had successfully hoodwinked their American “partners”, that the U.S. was asleep at the wheel while Canada quietly enriched The Cartels and hardened their monopolies, all with a sense of duper's delight. Unfortunately for them, the giant is awake and it’s not falling for the tricks anymore.
-
Now, we wait until the next time the poll is mentioned and Barky again claims it doesn't exist. A lot of posters here seem unable to correct their own mistaken beliefs. It's Belief Perseverance. The original lie "sticks" and they are unable to correct their thinking.
-
Very welcome. It has been a labor of love. Right now, there are a couple of new papers just published on the RNA:DNA hybrids, which contaminate the vials. Some vials/batches worse than others. Until this issue is resolved, all further mRNA vaccines invented will experience the same contamination. Dr. Kevin McKernan (SOLiD sequencing expert, R & D lead on The Human Genome Project with MIT/WIBR and the founder of Medicinal Genomics) was, if I remember correctly, the first to identify the DNA contamination. Later confirmed by about 8 independent labs. McKernan believes, in this new paper, that treating mRNA vaccines with a preparation of DNase I-XT during the manufacturing process may resolve the contamination issue. I am currently digesting and reviewing those papers before posting it on the Trickle Thread. But it seems very promising for making the mRNA technology safer. This is why we don't create vaccines and genetic therapy as "rush jobs". all this kind of testing would normally have been done BEFORE mass marketing. Dr. McKernan has developed a treatment for some of the worst vaccine-injured, with help from Japan and has recently started giving treatments there. Kayla Pollack, one of Canada's most severely injured, has been invited by Dr. McKernan (also a Canadian) to undergo the treatment in Japan. https://x.com/kcpollock/status/1794838685340361122?s=20
-
Ya, you keep accusing me of that, even though I have an 82-page thread on one topic with none of those things. Hundreds of peer-reviewed medical studies. I notice when someone posts something from social media, if it agrees with your preferred narrative, you have no problem with it then.
-
The poll has been removed now but there are still news articles about it. More than one in four Canadians support jail time for unvaccinated: poll | Regina Leader Post As the poll progressed, at the end it was over 60% of Canadians wanted their fellow citizens jailed. I have the final tally of the poll screenshotted somewhere, I'll try to find it if I have time.
-
Where did I say it was a flattering comparison?
-
This is the point I'm at. It's no longer incompetence or wrong intentions. At some point, you have to conclude it's been done on purpose.
-
I find it's very common on this board for certain posters to just quickly Google an opposite view and post it. They don't actually put any thought into evaluating opposing information. They don't think for themselves by considering how information fits into what is already known. In fact, a lot of them out-right refuse to read anything that is not their preferred narrative.
-
Where did I say that?
-
This was exactly the theme of Carney's speech in Davos. Only he added, "You all should hate him, too." I find it fascinating that all these elite parasites who have bankrupted the middle class in the biggest wealth transfer in human history and eroded democratic freedoms all over the world, can warn about Trump with a straight face. So far, the diversion from past Davos meetings is also fascinating: 1. Larry Fink admitted that the amount of energy needed for data centers cannot be derived from the intermittent power from wind & solar, they need steady baseload power because they can't be turned off & on. (Be prepared for energy rationing and our elderly freezing to death.) 2. They're not saying "stakeholders" anymore. They're back to "shareholders". 3. They've exchanged "climate change" with "weather change". Trump making his way to the forum in Davos:

-
Jody Wilson-Raybould announced she will be starting chemo for breast cancer shortly. https://x.com/Puglaas/status/2013394608508805156?s=20 I'm very sad to hear this news. She is one of the few politicians that I had utmost respect for. She stood up to Trudeau's corruption and lost her job for it.
-
Unfortunately, the helium deposits are mostly in Alberta and Saskatchewan, so Ottawa will never allow the industry to get too far. We have to accept that Canada's Net Zero fantasy means no industry in Canada. Especially if that industry is in the West. Fortunately, the helium deposits are mostly in Alberta and Saskatchewan and it's looking like we're gonna get the H. E. Double hockey sticks outta here.
-
I used to think calling these people deranged (as in Trump Derangement Syndrome) was going too far, but I don't anymore.