Goddess
-
Posts
6,312 -
Joined
-
Last visited
-
Days Won
78
Content Type
Profiles
Forums
Events
Everything posted by Goddess
-
 Faksova, K.; Walsh, D.; Jiang, Y.; Griffin, J.; Phillips, A.; Gentile, A.; Kwong, J.C.; Macartney, K.; Naus, M.; Grange, Z.; et al. COVID-19 vaccines and adverse events of special interest: A multinational Global Vaccine Data Network (GVDN) cohort study of 99 million vaccinated individuals. Vaccine 2024, https://doi.org/10.1016/j.vaccine.2024.01.100. Krumholz, H.M.; Wu, Y.; Sawano, M.; Shah, R.; Zhou, T.; Arun, A., S; Khosla, P.; Kaleem, S.; Anushree, V.; Bornali, B.; et al. Post-Vaccination Syndrome: A Descriptive Analysis of Reported Symptoms and Patient Experiences After Covid-19 Immunization. medRxiv 2023, 10.1101/2023.11.09.23298266, 2023.2011.2009.23298266. The toxic character of SARS-CoV-2 SP, despite its inability to replicate, is of more than theoretical concern. The newly published biochemistry paper reviews clinical studies that tracked markers of microvascular occlusion, including retinal vascular density and myocardial FDG uptake, with significant abnormalities persisting months after COVID-19 vaccinations. It also references a study of the health records of 99 million COVID-vaccinated individuals conducted by an international collaboration of 24 institutions, which found significantly increased incidences of myocarditis, pericarditis and other serious conditions [5]. Serious adverse effects were observed as well in a Yale study of 241 post-COVID vaccine syndrome patients [6]. On the other hand, the three generic drugs that gleaned the most attention as therapeutics for COVID-19 had a sound biochemical basis for efficacy, each significantly reducing RBC aggregation. The most distinct clinical benefits were observed for ivermectin, which neutralizes the virulence of SARS-CoV-2 SP by strongly binding to several sites on its N-terminal domain, competitively inhibiting its attachments to host cell glycans. In vitro, ivermectin not only blocked the SP-induced formation of RBC clumps, but it disaggregated such SP-induced RBC clumps within 30 minutes [2]. Three clinical studies demonstrated this rapid normalization of peripheral oxygen saturation (SpO2) in severe COVID-19 patients within 1-2 days after treatment with ivermectin, as reviewed in the newly published COVID-19 biochemistry paper and shown in the figure below, from that paper. Compounding the confusion about the biochemical mechanism of ivermectin, as the paper also notes, was the vulnerability of medical science to commodification, a subject that has engaged the contributions of some of science’s most distinguished scholars. Richard Horton, editor-in-chief of The Lancet, for example, wrote in 2015 that plagued by “flagrant conflicts of interest,” “much of the scientific literature, perhaps half, may simply be untrue” [8]. The rapidly expanding use of ivermectin to treat COVID-19 worldwide faced two streams of pushback by early 2021. One was a flurry of fabricated reports of ivermectin poisonings in the US reported in the major media worldwide, debunked and retracted, as exposed by the Washington Post [9] and other sources [10,11]. In one of the more imaginative of these fabrications, “gunshot victims” who were “left waiting as horse dewormer overdoses overwhelm[ed] Oklahoma hospitals” were shown waiting in line wearing winter coats, when temperatures that summer day ranged between 80° and 95° F. The set of charts and graphs below, based on data from the COVID-19 biochemistry paper and other sources [13,17-20], provides a reality check on COVID-19-related deaths before and after the nationwide deployment of COVID-19 vaccines in the US, and for those trends in Peru and Uttar Pradesh following the widespread distribution of ivermectin for COVID-19 prevention and treatment. A month before the US nationwide release of the Pfizer and Moderna COVID-19 vaccines on December 14, 2020 [19], the efficacy of both was touted to be 95% [21]. Yet COVID-19 deaths in 2021 actually increased by 18% from their 2020 total [17,18]. Excess deaths in the US were an identical 16% over projections from pre-pandemic levels for both the years 2020 and 2021 [13]. These data align with a conclusion expressed in a 2023 paper by Anothy Fauci and two other NIH scientists, that “none of the predominantly mucosal respiratory viruses,” including coronaviruses, “have ever been effectively controlled by vaccines” [22]. In Peru, excess deaths decreased 14-fold between August 1 and December 1, 2020, concurrent with a massive, nationwide distribution of ivermectin that began in August 2020. Then, after a new president was elected on November 17 who restricted the use of ivermectin, excess deaths increased 13-fold from December 1, 2020, to February 1, 2021. Although correlation does not necessarily imply causation, a rigorous state-by-state analysis of ivermectin use in Peru’s 25 states using national health data that aligned with WHO summary data (the same data source as for the chart above) showed that in this case, ivermectin clearly caused the reductions in deaths observed. The analysis found a correlation between the extent of ivermectin use and reductions in excess deaths, by state, with p < 0.002, and no indication of any significant effect by several potential confounding factors considered [20]. In Uttar Pradesh, the largest state in India, having a population of 229 million, COVID-19 deaths fell by 97%, between May 7 and July 7, 2021, after a mass distribution of ivermectin, doxycycline, zinc with vitamins and acetaminophen tablets that began on May 5, 2021. The cumulative total of COVID-19 deaths per million population in Uttar Pradesh from July 7, 2021, to April 1, 2023, was 0.27% of that figure in the US for the same period [20]. In conclusion, when claims that ignore fundamentals of biochemistry but remove barriers for profitable new therapeutics are advanced in the name of science, not only public health but the fabric of civilization is undermined. It is hoped that the lapses illuminated here can be rectified and associated opportunities embraced.
Faksova, K.; Walsh, D.; Jiang, Y.; Griffin, J.; Phillips, A.; Gentile, A.; Kwong, J.C.; Macartney, K.; Naus, M.; Grange, Z.; et al. COVID-19 vaccines and adverse events of special interest: A multinational Global Vaccine Data Network (GVDN) cohort study of 99 million vaccinated individuals. Vaccine 2024, https://doi.org/10.1016/j.vaccine.2024.01.100. Krumholz, H.M.; Wu, Y.; Sawano, M.; Shah, R.; Zhou, T.; Arun, A., S; Khosla, P.; Kaleem, S.; Anushree, V.; Bornali, B.; et al. Post-Vaccination Syndrome: A Descriptive Analysis of Reported Symptoms and Patient Experiences After Covid-19 Immunization. medRxiv 2023, 10.1101/2023.11.09.23298266, 2023.2011.2009.23298266. The toxic character of SARS-CoV-2 SP, despite its inability to replicate, is of more than theoretical concern. The newly published biochemistry paper reviews clinical studies that tracked markers of microvascular occlusion, including retinal vascular density and myocardial FDG uptake, with significant abnormalities persisting months after COVID-19 vaccinations. It also references a study of the health records of 99 million COVID-vaccinated individuals conducted by an international collaboration of 24 institutions, which found significantly increased incidences of myocarditis, pericarditis and other serious conditions [5]. Serious adverse effects were observed as well in a Yale study of 241 post-COVID vaccine syndrome patients [6]. On the other hand, the three generic drugs that gleaned the most attention as therapeutics for COVID-19 had a sound biochemical basis for efficacy, each significantly reducing RBC aggregation. The most distinct clinical benefits were observed for ivermectin, which neutralizes the virulence of SARS-CoV-2 SP by strongly binding to several sites on its N-terminal domain, competitively inhibiting its attachments to host cell glycans. In vitro, ivermectin not only blocked the SP-induced formation of RBC clumps, but it disaggregated such SP-induced RBC clumps within 30 minutes [2]. Three clinical studies demonstrated this rapid normalization of peripheral oxygen saturation (SpO2) in severe COVID-19 patients within 1-2 days after treatment with ivermectin, as reviewed in the newly published COVID-19 biochemistry paper and shown in the figure below, from that paper. Compounding the confusion about the biochemical mechanism of ivermectin, as the paper also notes, was the vulnerability of medical science to commodification, a subject that has engaged the contributions of some of science’s most distinguished scholars. Richard Horton, editor-in-chief of The Lancet, for example, wrote in 2015 that plagued by “flagrant conflicts of interest,” “much of the scientific literature, perhaps half, may simply be untrue” [8]. The rapidly expanding use of ivermectin to treat COVID-19 worldwide faced two streams of pushback by early 2021. One was a flurry of fabricated reports of ivermectin poisonings in the US reported in the major media worldwide, debunked and retracted, as exposed by the Washington Post [9] and other sources [10,11]. In one of the more imaginative of these fabrications, “gunshot victims” who were “left waiting as horse dewormer overdoses overwhelm[ed] Oklahoma hospitals” were shown waiting in line wearing winter coats, when temperatures that summer day ranged between 80° and 95° F. The set of charts and graphs below, based on data from the COVID-19 biochemistry paper and other sources [13,17-20], provides a reality check on COVID-19-related deaths before and after the nationwide deployment of COVID-19 vaccines in the US, and for those trends in Peru and Uttar Pradesh following the widespread distribution of ivermectin for COVID-19 prevention and treatment. A month before the US nationwide release of the Pfizer and Moderna COVID-19 vaccines on December 14, 2020 [19], the efficacy of both was touted to be 95% [21]. Yet COVID-19 deaths in 2021 actually increased by 18% from their 2020 total [17,18]. Excess deaths in the US were an identical 16% over projections from pre-pandemic levels for both the years 2020 and 2021 [13]. These data align with a conclusion expressed in a 2023 paper by Anothy Fauci and two other NIH scientists, that “none of the predominantly mucosal respiratory viruses,” including coronaviruses, “have ever been effectively controlled by vaccines” [22]. In Peru, excess deaths decreased 14-fold between August 1 and December 1, 2020, concurrent with a massive, nationwide distribution of ivermectin that began in August 2020. Then, after a new president was elected on November 17 who restricted the use of ivermectin, excess deaths increased 13-fold from December 1, 2020, to February 1, 2021. Although correlation does not necessarily imply causation, a rigorous state-by-state analysis of ivermectin use in Peru’s 25 states using national health data that aligned with WHO summary data (the same data source as for the chart above) showed that in this case, ivermectin clearly caused the reductions in deaths observed. The analysis found a correlation between the extent of ivermectin use and reductions in excess deaths, by state, with p < 0.002, and no indication of any significant effect by several potential confounding factors considered [20]. In Uttar Pradesh, the largest state in India, having a population of 229 million, COVID-19 deaths fell by 97%, between May 7 and July 7, 2021, after a mass distribution of ivermectin, doxycycline, zinc with vitamins and acetaminophen tablets that began on May 5, 2021. The cumulative total of COVID-19 deaths per million population in Uttar Pradesh from July 7, 2021, to April 1, 2023, was 0.27% of that figure in the US for the same period [20]. In conclusion, when claims that ignore fundamentals of biochemistry but remove barriers for profitable new therapeutics are advanced in the name of science, not only public health but the fabric of civilization is undermined. It is hoped that the lapses illuminated here can be rectified and associated opportunities embraced. -
Before my recent hiatus from here, he did confess that he is only here on this forum to troll, that he gets a huge kick out of it. Sad and empty person, best ignored. He adds nothing to any discussion.
-
Post after post after post, of nothing but whining, accusing others of whining. 🙄
-
Stop me if any of this starts to sound familiar. 😄 It's 1918, and the Spanish Flu seems to be killing otherwise young and healthy people (especially soldiers) in a matter of days. They would be a bit sick, then suddenly die of massive organ failure and “wet hemorrhagic lungs.” The progression was incredibly fast, seemingly irreversible, and was stacking people who really ought to have been low risk in mortuaries like cordwood. If it could do this to a soldier in his prime in a matter of days, every last one of us should be terrified. But did you know......? There is actually quite a lot of convincing evidence that many of the “young, healthy deaths” of Spanish Flu were iatrogenic? Iatrogenic death is when the doctor kills you. And there is a long and unpleasant history on that one - from Benjamin Rush bleeding George Washington to death, to killing “witchy” cats to stop a plague carried by the fleas of the very rats they were eating, to (and especially) new “wonder drugs” that are poorly understood but that rapidly go into widespread use. And one of those drugs - during the time of the Spanish Flu - was aspirin. Aspirin had just come into widespread availability in 1918. And Bayer was rushing it to market for the pandemic. It was the new wowie-zowie drug and doctors (and especially militaries) all over the world fell in love with it. They prescribed it widely to those with Spanish Flu. In doses ranging from 8 to 31 grams per day. Oopsie doodle. A typical aspirin today is 325mg and max dosing per day is ~4 grams. A toxic dose is about 20g for a 180 pound person. 31g is “you’re going to die really, really fast and there is not a damn thing anyone can do to stop it once you take that dose.” This is why incredible caution should be exercised around large departures from tested and true medical practice and new pharma modalities and products. This case fatality rate has never looked even remotely plausible for flu. You simply do not get a respiratory disease like that in a modern (or possibly any) society, especially not in young, healthy people. It’s just not a thing. But widespread poisoning by well meaning medical professionals who have no idea how dangerous the products and procedures they are playing with - is. "Official recommendations for aspirin were issued on 13 September 1918 by the US Surgeon General [64], who stated aspirin had been used in foreign countries “apparently with much success in the relief of symptoms” (p 13), on 26 September 1918 by the US Navy [29], and on 5 October 1918 by The Journal of the American Medical Association [31]. Recommendations often suggested dose regimens that predispose to toxicity as noted above. At the US Army camp with the highest mortality rate, doctors followed Osler’s treatment recommendations, which included aspirin [48], ordering 100,000 tablets [65]. Aspirin sales more than doubled between 1918 and 1920 [66]." Consider the below quote from HHS (1918). And this is not some “quaint delusion of doctors that wise men of modern medicine have exceeded and no longer fall prey to.” This EXACT mindset was a massive killer in covid: VENTILATORS. “Vent early, vent hard” - It ran riot in New York and many other parts of the world. It was used not just to treat patients but to “protect doctors” under the misbegotten theory that an intubated patient would not spread covid and that “doctors needed to be protected.” There was a whole national campaign to build more ventilators. Patients were intubated when they should not have been. When this failed to work, they kept turning up the pressure on the vents. And this killed people wholesale. Ask the frontline nurses and doctors who quit or were fired because their consciences would not allow them to continue killing people and no one would to listen to them. That’s not covid death. That’s iatrogenic death. Once NYC figured out that vents were killing people in droves and switched to proning as others had done, this death rate dropped. But an awful lot of people had lost their lives by then. And, as in Spanish Flu, this high death rate was used as a pretext for more aggressive and ill considered actions that drove more iatrogenic death. It’s a vicious cycle and once it gets going, it’s self-feeding. Every time you inadvertently kill people out of ignorance or fear, it makes the purported pathogen look more deadly and drives you to new “reactions” and mis-calibrations where you once more kill people. It’s not like this was unknown or unknowable. But most countries just plain forgot and did the wrong thing, despite what they knew. Sometimes failing the Asch Conformity test is fatal to those around you. But once you lose your mind, start over-reacting, and act from fear or twisted interest, it takes on a life of its own. We really need to stop presuming that high excess death = proof of bad virus and start asking the serious questions: how much of it was iatrogenic? how much came from the insane policies of scaring people away from doctors and medical treatment? how much from barring access to longstanding effective drugs and treatment in favor of new ones that mostly failed spectacularly and killed people? how many deaths of despair were caused among the alone and isolated in care homes? how many deaths in hospitals because patients were denied the ability to see family and perhaps more importantly because friends and family were denied the ability to be there for their loved ones to serve as advocates and organizers? (if you have ever been in hospital or been there to protect those close to you from one and make sure sound and sufficient care is supplied and applied you know what i mean on this. a hospital is no place to be alone and helpless.) how many killed by vents, by bad nursing home policy, by putting “saving hospitals” above “saving people” and by “wonder drugs” that failed to live up to billing and whose side effects were not taken into account? to what extent was the “covid pandemic” just a replay of spanish flu where much, probably most of the fatality rate was from bad response rather than truly bad virus? Please don’t misunderstand: I am NOT arguing that covid did not kill anyone or at least pull forward some deaths that likely would have occurred soon afterwards, shortening lives by weeks and months (but not years) and thus causing spikes in deaths. Many other flus had far higher CFR than covid did. The Asian flu in 57-8, the Hong Kong flu of 68, the flu of 76 (whose vaccine was such an infamous problem), H1N1 in 2009 - none of these were more than a tiny ripple. Not zika, not dengue, ebola, or bird flu. None of it. Every couple years, a new one is trotted out in search of a crisis. It’s a gold mine for Pharma. And it will be trotted out again. These were all spectacular nothing-burgers. Sure, sometimes we get one that’s a bit worse, but even a “bad pandemic” really does not move the needle much in the antibiotics era. Never has. The only 2 really nasty ones in Amercian history were Spanish Flu and SARScov-2 and both appear to have had an awful lot of their excess death toll driven by bad response rather than bad virus. We know covid was circulating in late 2019. It was a nasty bug. getting it was unpleasant. but it wasn’t killing people in unusual numbers until the panic started. Then, suddenly, it was. Again, I'm not saying it would not have led to any excess deaths had we not panicked and done all manner of poorly conceived things that led to iatrogenic deaths. The question is “how much?” And the answer might well be “quite a lot less than people commonly suppose.” The answer might well be “so little that had we not named and obsessed over it, few would have really noticed.” It's the desire to “do something” and “appear active and on top of it” that crashes into a horrifying tendency to crisis profiteer, where we suddenly lose our collective minds and run off in wild directions embracing terrible ideas and eschewing those long shown effective that does this. And that’s how people die. Needlessly. If we would not re-live this in the future, it is in the resistance to fear that our resiliency lies. This is why the exploration of just what was done, by whom, why and to what effect is vital. But historically, pandemics in the modern age simply are not dangerous. Unless you panic.
-
You, too, Moonie. When studies are posted that show the spike/LNPs in the ovaries and testes and adults discuss the possible implications of toxins navigating their way to human reproductive organs, you two HAHAHA'ing about it, makes me pity you. It must be hard going through life without the intelligence to comprehend the implications of things like that.
-
ExF and Moonie always remind me of those annoying kids who run around screaming and yelling and knocking shit over: "Everyone pay attention to Meeeeeeee!" while adults are trying to have a conversation.
-
ExFlyer, I'm sure you think by putting the HAHAHA emoji on everything I post, that you are somehow "getting to me". You're not. I kind of think of you as the mental patient sitting in the corner, rocking and giggling, too unintelligent to understand what's going on around him. I know you do it for attention and acknowledgment. Consider yourself "acknowledged."
-
That's the million dollar question. We don't know. And the scientists and researchers who are trying to find out how bad it is, so that we can work on finding help for people, are continually being shot down and silenced by media, gov't, Big Pharma and their useful idjits like the ones here, who are against finding out. What we do know - excess deaths in highly vaxxed countries are far more than covid deaths ever were and this is being ignored. The #1 reason for death in Alberta is "unknown cause". We do know the spike and the LNPs are settling primarily in the ovaries and testes. What that means for future generation's fertility, time will tell. But it's likely not good.
-
It does. I posted links to these studies in the Trickle thread. I'm impressed you know to ask about this - crossing the BB is a HUGE no-no and yet when it was reported - there was a collective "Meh...." Ya, the war on IVM was astonishing to me. I had been given a prescription for it years ago, during my traveling years. There is quite the story about how its use was demonized and suppressed- if you're interested, (let me know if you can't find it through Google) you should check out these names: Dr. Tess Lawrie, Andrew Hill, Andrew Owen. I find you very refreshing. Not many people questioned anything. Wow, you've hit nearly all the major issues. Again, I tackled prion diseases and posted the studies in the Trickle thread.
-
Two words for you: OPIOD CRISIS
-
Honestly, even if I had taken the jabs, I would still be very interested in the studies that followed because they were experimental and using novel platforms (mRNA and LNP delivery).
-
Hahaha No. No, they don't. You've asked me this a few times before. No. I'm more of an "anti-being-forced-to-take-an-experimental-injection-without-any-long term-studies-especially-when-my-risk-is-below- 0.02%" type of person.
-
DNA damages occur within our body, especially during cell division - which happens in us all the time. As we get older, or as we get exposed to stresses (like consuming lots of processed foods), DNA damage is increased in our body. Thankfully, most of us have working P53 genes that activates whenever it detects any DNA damages. P53 basically tells the cells to STOP dividing, repairs the DNA damages and then green lights the cells to start dividing again! When P53 detects that DNA damages are too much, it instructs the cells to go kill themselves instead of replicating further. It’s like a very cool repair engineer in our body, keeping DNA damages at bay before they develop into cancer. Dr. Wafik El-Deiry (Brown University) is considered on of the most prominent leading figureheads in P53 gene research. His work in P53 gene research goes all the way back to 1992. Dr. El-Deiry found out how the P53 protein, which helps prevent tumors, attaches to our DNA. This important finding, shared in the journal Nature Genetics in 1992, has helped us understand which genes are directly influenced by P53 to stop cancer growth. He discovered a gene named P21, which P53 affects. P21 acts like a brake in our cells, slowing down their division, especially when they're under stress. What did Dr. El-Deiry discover? Essentially, he uncovered that the spike protein blocks the P53 gene's function. 😟 Does this imply that everyone will develop cancer? Not necessarily. However, without the protective action of the P53 gene, the likelihood of cancer rises significantly, especially in those with more DNA damage. We know now that the spike protein continues to be produced non-stop, so....that's not good. SARS-CoV-2 spike S2 subunit inhibits p53 activation of p21(WAF1), TRAIL Death Receptor DR5 and MDM2 proteins in cancer cells | bioRxiv Increases in cancer following covid vaccination has already been confirmed by the japanese: 20240408-14533-1avkjxd.pdf (cureus.com) And Dr. Maarten Fornerod, a respected Dutch cancer researcher and molecular biologist concurs. Dr. M.W.M. (Maarten) Fornerod - Principal Investigator - Erasmus MC (Further investigation, which eyeball is against.) Explained further in Dr. Rose's substack, here: (Although I warn you - she's a super smarty-pants and it takes effort to comprehend her.) (17) S2 of SARS-2 spike buggers up p53 - by Jessica Rose (substack.com)
-
Yes, which is why so many countries have stopped giving them to teens and young adults. But eyeball seems unable to assimilate new info or connect new info to old info.
-
Yes, that was my point - there is much newer research on this. Seems it's you it's stuck in the past. Why are you against doing studies on these jabs?
-
You should really check who funds the studies, too:
-
I glanced at this and don't see a date on this article, but I see the research ends sometime in 2022. I posted much more recent studies on myocarditis after covid vax in the Trickle thread. This article is extremely out-dated. Sort of what happens when you just do a quick google, instead of actual research. 🙄
-
Did you know that the lipid nanoparticles (LNPs) used to make Moderna’s and Pfizer’s shots were re-purposed to serve as vaccine platforms? They were originally intended to be a delivery mechanism for drugs and/or gene therapies. The reason LNPs were rejected as a platform, is that the LNPs were toxic if administered multiple times. And treatment of cancers and other diseases with LNPs required multi-dosing protocols. For this reason, several companies abandoned the use of LNPs. But Moderna decided to change course and use LNPs as a vaccine delivery system. Why? Because they understood that an ideal vaccine is one that requires a single dose. Here is Health Canada’s official definition of an ideal vaccine here: So, problem solved. A good LNP-based vaccine would require only a single dose. No multi-dosing = none of the toxicities known to be associated with multiple administrations of LNPs. Compare to Stéphane Bancel's comments, CEO of Moderna, which was published on September 13, 2016. Note his serious concerns about the LNPs that his company is using: “Delivery – actually getting RNA into cells – has long bedeviled the whole field. On their own, RNA molecules have a hard time reaching their targets. They work better if they’re wrapped up in a delivery mechanism, such as nanoparticles made of lipids. But those nanoparticles can lead to dangerous side effects, especially if a patient has to take repeated doses over months or years. Novartis abandoned the related realm of RNA interference over concerns about toxicity, as did Merck and Roche.” It's not just the spike protein (which there is no mechanism in the jabs to stop your body from producing) that is toxic. The LNPs are, as well. (But I'm sure it's just the breakfast food thing that eyeball thinks.) You can go see it on their website. It's the JCCF - the lawyers who won the Emergency Act case against Trudeau.
-
Microsoft Word - The rise of excess and unexplained deaths in Canada_FINAL.docx (jccf.ca) ^^^ Canada, not Spain ^^^ And only covering up to 2022
-
I think we've covered the sketchy way "covid deaths" were counted, quite a few times. Remember the 14 year old boy in AB with terminal brain cancer who was "tested" for covid while in a coma, hours before his death and thus....counted and announced as a covid death?
-
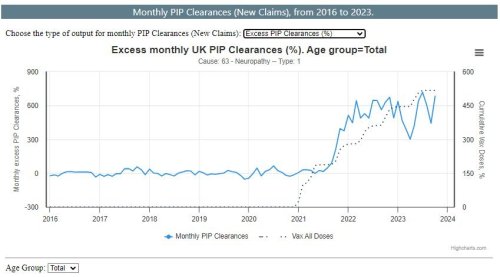
So, according to the eyeball, there is a 0% chance that the UK's 680% with a z-score of 19 spike in neurodegenerative diseases, is caused by millions of people being forced to inject an experimental vax with no long-term studies and that the more likely culprit is a change in people's breakfast food choices. No need to investigate. Well, I'm reassured. Are you?
-
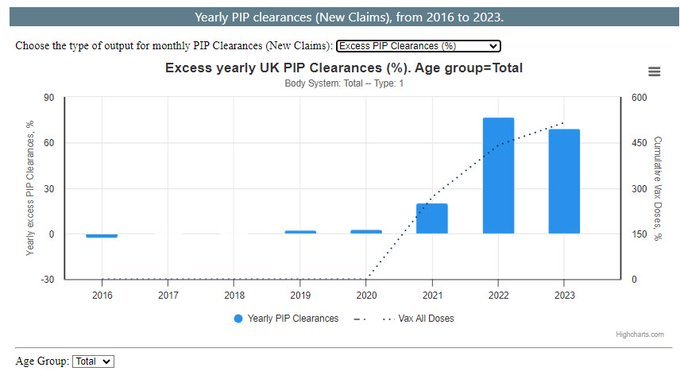
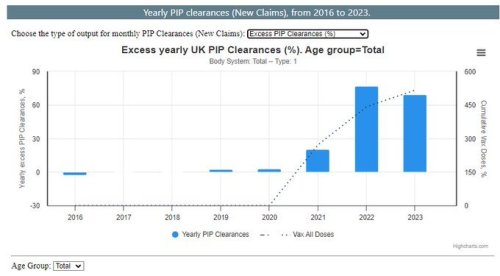
This is some UK data recently posted: Excess NEW Neuropathy claims in UK are up 680% as of October 2023, started to rise in 2021. A Z-score of 19. Is a 680% rise in claims with a z-score of 19, a lot? In case you are interested, Total NEW excess disability claims for all body systems in the UK were up: 2.4% in 2019 2.9% in 2020 20.5% in 2021 76.7% in 2022 69.1% in 2023 Did I mention Z-scores? Yes, I did.
-
Weird how so many health conditions and excess deaths have sky-rocketed since the vax rollout, though. I'm sure it's just a coincidence.......