Goddess
-
Posts
10,058 -
Joined
-
Last visited
-
Days Won
93
Content Type
Profiles
Forums
Events
Everything posted by Goddess
-
 The only reason they're getting away with it is because Jim Flaherty is dead.
The only reason they're getting away with it is because Jim Flaherty is dead. -
Polievre has spoken on how Canada can help in reducing GLOBAL emissions in multiple interviews. Carney thinks more money in billionaire's pockets and impoverishing the rest of the planet reduces emissions. You decide. It sounds like you believe the latter.
-
I know he's wrong. I'll try to find it but there has been a couple of times on this planet when CO2 level rose dramatically and there was zero chance of MAN being the culprit. Climate alarmists don't look at the entire history of the planet. They look at one tiny window - thus, the hysteria.
-
That's not what Polievre has said. He's actually explained how the Conservatives plan to cut GLOBAL emissions in multiple interviews. That's the difference. Libs claim that taxing Canadians will cut Canada's emissions - it hasn't. But they don't talk about how Canada can cut GLOBAL emissions. Is this a GLOBAL problem or is it a Canada problem? Conservatives are thinking bigger than Libs on this one.
-
I'm surprisednotsurprised that so many Lib supporters don't recognize the same "instill fear and conquer" diversionary tactics that were used during c0v1d. Trump & the tariffs, while important, pales in comparison to Canada's stagnation for the last 10 years. And the Lib progressive policies that have created social chaos in the form of a divided society, lax judiciary, widespread drug use and homelessness, rampant mass immigration, healthcare crises...... Carney keeps hammering Trump!, Trump!, Trump! with very little about the problems that will still be around long after the tariffs are dealt with. I hear vague promises about "building back our economy". With what?? Libs have stymied any growth for 10 years. We are missing pipelines and entire industries.
-
I feel like, as more and more people catch on to the climate scam, they're trying to walk back some of the hysteria now. I'm hearing and seeing more of the phrase "climate variability". That the climate varies, is apparently, an epiphany.
-
So, rather than speak to Trump and work on new trade agreements, it's better to cut off the Americans and no longer be an ally? Burn all the bridges? That's the solution? Gawd, Liberals are always so EXTREME.
-
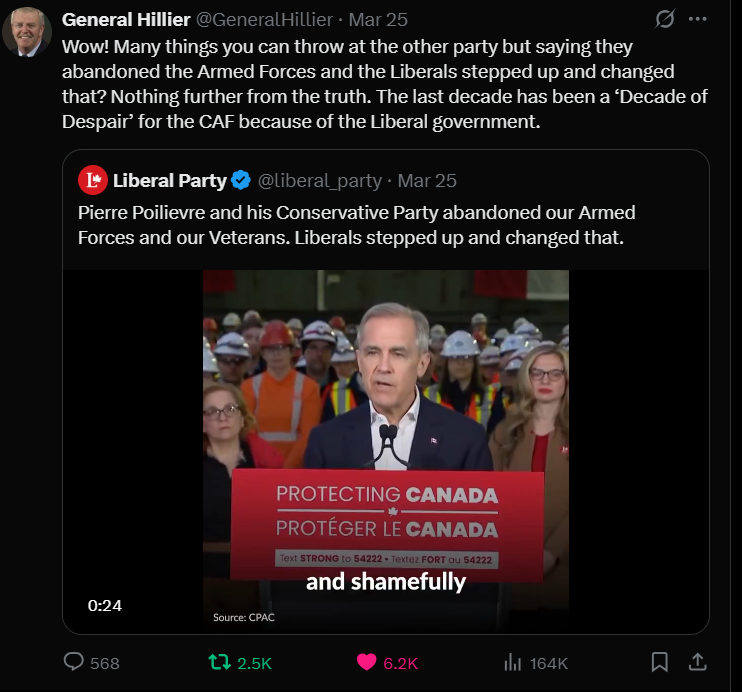
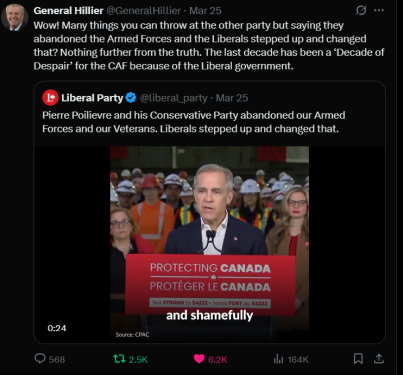
How a caretaker government functions in the middle of a trade war | CBC News In the Westminster parliamentary system used in Canada, the legitimacy of an elected government hinges on its ability to command the confidence of the House of Commons. During an election period, the House is shut and so the prime minister cannot seek approval from the elected chamber. Because of that, the prime minister and cabinet are directed by the convention to act with restraint, which means they shouldn't introduce big, new things or make changes that would be onerous for the next government to roll back. There are also some guidelines for how government advertising and communicating takes place. The central principle is that all communication should be non-partisan, and be limited to messages about public health, safety or urgent business. Carney is not elected and with one statement he's trying to change the entire course of the North American geopolitical relationship that's been in place for over 80 years. This is exactly what Polievre has been warning about him.
-
He has no mandate to unilaterally make this decision. He's not in a boardroom talking about a corporate takeover, where it's only dollars & cents at stake. What politicians say affects the stock market. Has he not seen the state of our military? We barely have one. And why should he care? He moved all his money out right before this. Just so we're clear - Carney has not even talked to Trump yet. And he just declared it OVER. At a time when the Americans have been very concerned about Canada's ties to China, He just told Trump that Canada is not an ally anymore. This guy is a lunatic.
-
China and Russia are high-fiving and jumping for joy along with you.
-
They have to force people to stand there? 🤣

-
Congress has to OK invading Canada. That's not going to happen. Then the US military also has to follow an order to invade Canada. Also not going to happen. The Us citizens would not allow an invasion of Canada. As I've said before, I take Trump seriously, but not literally.
-
Haha, there's this one, too:
-
That was a weird one, considering they are always going after PP about not getting his security clearance. I mean, what good is it, really, if Carney has it and still is not privy to any information?
-
From Mark Oshinkie's substack today: GET VAXXED, DIE ANYWAY During early Coronamania, many stated a strong, but seemingly insincere, desire to “save grandma.” Yet, several weeks before lockdowns began, college students were saying “OK, Boomer” to show disdain for those old and in the way, i.e., those over 50 who may have expressed some non-PC perspective. I don’t watch or read much news. I first heard about “the Coronavirus” in the first week of March, 2020, when a student who worked for me spoke laughingly of a new microbe that her generation had dubbed “The Boomer Remover.” Within a week, the government and media had built a plainly bogus but widely accepted—including by most college students and graduates—narrative that some “novel” virus threatened everyone. Most were conned into hiding from others so as to avoid being “super-spreaders” who might bring The Virus home to grandma/pa; even though very few American grandmas/pas shared living quarters with those under 50. In general, the Scamdemic has been based on convincing a gullible, mathematically illiterate, illogical, fearful, groupthinking public that exceptions were the norm. It turns out that this task was easy. Read More: GET VAXXED, DIE ANYWAY - by Mark Oshinskie
-
I feel like this could possibly be an "on purpose" leak. Europe fumes at Trump team’s insults in leaked Signal chat – POLITICO There was no actual intel in it and all it seemed to do was pi$$ off the Europeans because it mostly just insulted them. Vance had just been to the EU and told them they needed to start coughing up more for their own security and stop relying on the US. “British and European officials and diplomats,” Politico explained, “reacted with a mix of hurt and anger.” It woefully added, “in Europe, the tone among diplomats was more of grief and resignation.” Poor little diplomats. Why don't they just shrug their shoulders and say, "Who cares what those American m0r0ns think?" “An EU diplomat noted it underlined the impression that Vance was the driver of U.S. hostility towards Europe.” They are suddenly taking the Vice President a whole lot more seriously. In one harmless leak, the Europeans have been convinced that Trump is serious, in a profound way that no public statement could ever have achieved: Mission accomplished.
-
HOLY 💩!! While Parliament is dissolved, Carney - the unelected 10-day old caretaker PM - just unilaterally declared that Canada's 157-year long relationship with the US is.......OVER.
-
In reality, it was mostly the Millennials and teens still living at home who couldn't work a summer job because of c0v1d that bilked the CERB program to the tune of $3 billion in wrongful payments, so...... Liberals didn't give a rat's patootie if claims were legit and mostly refused to recoup from people who cheated the system, so now everybody pays.
-
This election is definitely Boomers, who want to keep the status quo, VS. Younger People, who need change. I see a lot of comments on news articles like these ones: laura MXXXXXX-jXXXXX older folk here and this is my take , I just don`t care about your choice. Im good with any of them. I can sit back and not care because I made smart choices when I was younger and I had ambition and sacrificed some fun times for my future. It paid off, nope I`m not filthy rich, my house is not worth a fortune but I'm comfortable. laura MXXXXXX-jXXXXX I can agree with you 100% i did the same to secure my future and living comfortably without the handouts and I am not RICH PERSON EITHER unfortunately its the old boomer population (> 60) voting and supporting these lieberals.. The boomer arent feeling or understanding the financial, domestic and health issue under 50 age adults are facing.... being a large portion of the population they will have an impact.. Insane This feels very much like, "I got mine when times were good, so F*&%K the rest of you."
-
Not real sure about that. The economy still seems to be what normal people are worried about. It's only the Libs that keep trying to make Trump the main issue in this election. And I think this is going to cost them in the end. Again, they don't' listen and are completely out of touch with what normal Canadians' concerns are.
-
Mass immigration AND net zero is not possible.
-
Or they could use one of these:

-
For the Lib supporters here, honest question: What about the last 10 years has been so utterly fabulous FOR CANADIANS AS A WHOLE, NOT JUST ONE AREA OF CANADA, that you want more of it? I mean, our resources have been squandered to the point the US is bullying us, Trudeau invested all our money into EV's and battery plants that have mostly fled with our money, tent cities everywhere, drug epidemics, violent criminals and pedophiles let out into our streets, the longest list of insider trading and ethical violations, government waste was off the charts....it's endless the amount of scandals and during it all, the Libs focus was getting tampons into men's bathrooms. I mean, holy crap, even they admit they boffed immigration, they boffed housing, they boffed the economy. These are basic things, people. And all of them running for leadership said "Ya, we weren't listening to Canadians, but we're going to now." Holy crap! How is that an epiphany in a DEMOCRACY? What about any of this says, "We need lots and lots more of everything we've gotten for the last 10 years."
-
I blame Trump.
-
I don't know what happened there 🤣 it was very weird.